
There are situations where an air-bone gap (ABG) can lead to one ear being under-aided; using some idealised examples this document illustrates when this might occur and how to avoid it. Although Starkey Inspire software was used to illustrate this issue, a similar situation exists with other manufacturers’ software.
Consider the audiogram below (left) prior to masking. When masked, there are several potential outcomes; one such outcome is shown to the right. In this simplifed example, the hearing loss on the left ear was found to be purely sensori-neural.
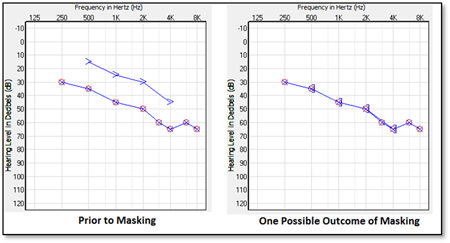
At this point we can deduce that the right ear has a mixed loss with a conductive element of approximately 20dB. As the client will have already endured a significant period of masking; is it appropriate to perform additional masking to confirm what we already know concerning the hearing loss on the right side? The source for the original BC data prior to masking can only have been the right cochlea.
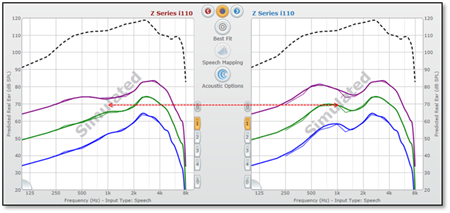
In order to ensure the right ear is not under-aided, it is essential that BC data is entered so that the additional gain necessitated by the air-bone gap can be applied. The Predicted Real Ear Response (in dBSPL) with and without the air-bone gap data are shown below. Note the approximate 5dB reduction in gain without taking the ABG into account. There are also changes in the compression ratios.

Therefore, to ensure an accurate gain target, either enter the original not masked BC data on the right audiogram (and save to NOAH with the comment “Audiogram for programming purposes”) or carry out masked BC measurements for the right side.
If matching to REM targets, there is another variable – the behaviour of the REM software itself; in theory, this should be similar but should be verified for your chosen REM system.
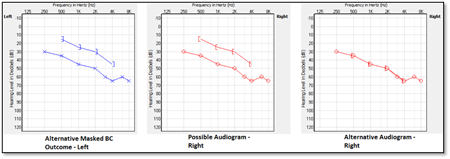
There is of course another possible outcome once the masked BC thresholds for the left ear have been determined; an air-bone gap may be present for this ear. Indeed there may be no significant change at all in the measured values (as illustrated below left). In this case we can draw no conclusions for the right ear; we have no choice but to measure the masked BC thresholds for the right cochlea.
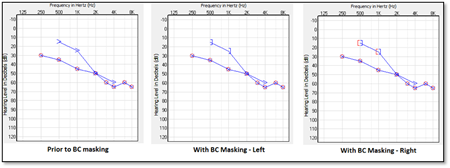
There is another factor that must also be taken into account. Consider the audiograms below; masked BC for the left ear confirms a 20dB air-bone gap in the low frequencies (left-hand and centre audiograms). Consequently we need to obtain masked BC data for the right ear – but only at 500Hz and 1kHz.
We already know there is no air-bone gap on the right at 2kHz and 4kHz as we have already determined the BC threshold of the better cochlea from the measurements on the left ear. As the BC thresholds cannot be any more acute than this, for either cochlea, we cannot have an air-bone gap at these frequencies.
Assume for the moment that an air-bone gap is present on the right ear in the lower frequencies (as illustrated by the right-hand graph below). In this example, we would naturally expect to see REM or fitting software calculate similar targets for both ears.
However, we now have a situation where we have four BC measurements for the left ear (either masked or not) and two for the right. The screenshot below shows the targets (Predicted Real Ear Response in dBSPL) as calculated by Inspire; note the reduced gain on the right ear in the low frequencies.
In order for BC data to be taken into account in calculating the target gain, at least three measurements are required for the ear in question. In this case the best practice is to create another “Audiogram for programming purposes” and copy the 2kHz and 4kHz BC data from the left to the right ear.
It is worth experimenting with other manufacturers’ fitting and REM software to confirm their behaviour under such circumstances.